Why Different Approaches Exist
Trauma affects people in many ways. For some, it shows up in the body, as tension, exhaustion, or feeling “on edge.” For others, it shows up in thoughts, emotions, or relationships. Because trauma touches both body and mind, different therapies have developed to meet people where they are.
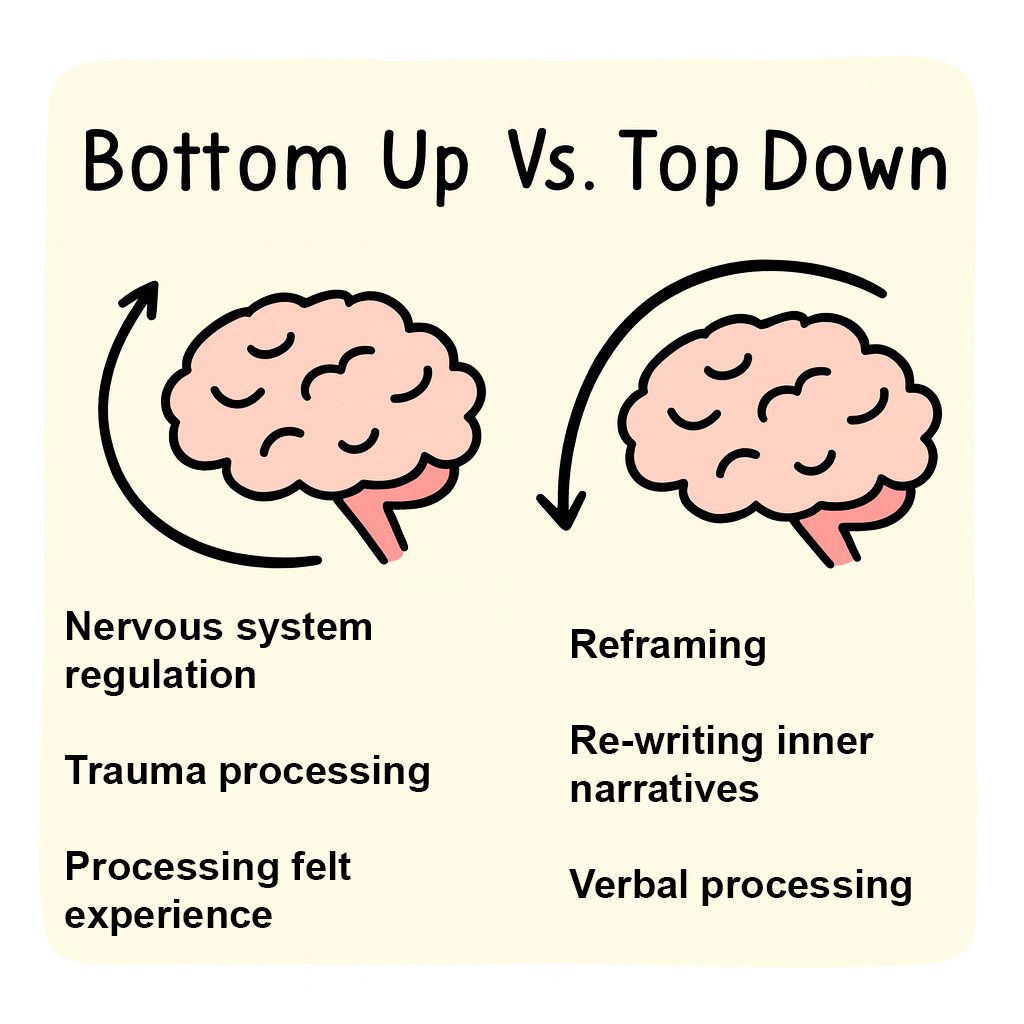
Some therapies work mainly “from the body up” (known as bottom up), helping the nervous
system calm, regulate, and find safety again. Others work “from the mind down” (known as
top down), helping us put words to what happened, make sense of it, and re-shape our beliefs.
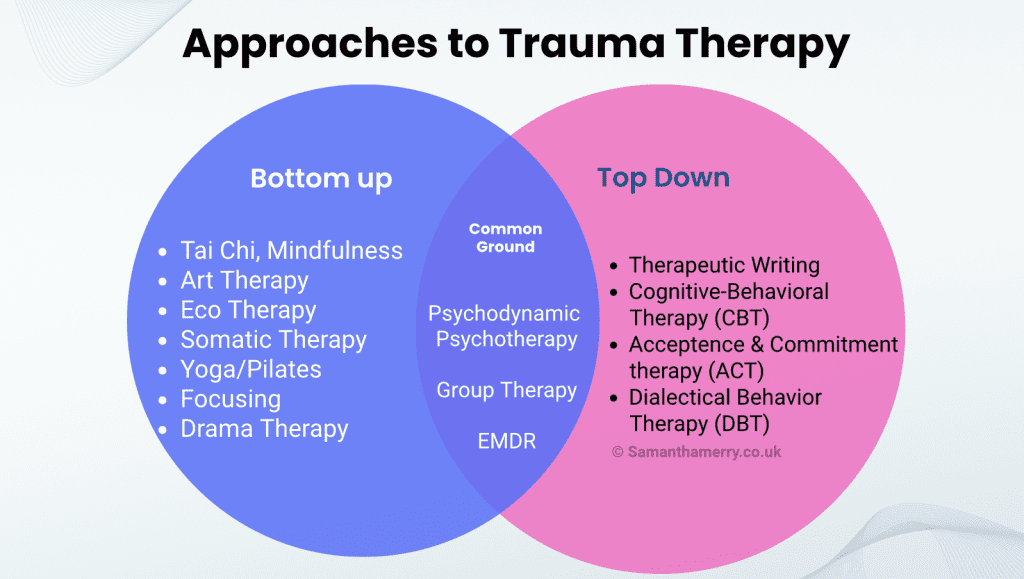
Many approaches, including psychodynamic psychotherapy, do both.
There isn’t one “right” therapy for trauma. Sometimes one approach is what’s needed, and at other times a combination is most helpful. Healing can be a journey of trying different ways of working until something feels like a good fit.
Top-Down and Bottom-Up: A Useful Framework
Therapies for trauma are often described as working either from the top down or from the bottom up. Top-down approaches work primarily through language, cognition, and meaning-making, helping you put words to what happened, reframe beliefs, and understand your responses. Bottom-up approaches work primarily through the body and nervous system, helping to regulate arousal and restore a sense of safety before moving into narrative or cognitive processing.
Most experienced trauma therapists draw on both, and the distinction is a starting point for understanding rather than a rigid category. What matters more than where an approach begins is whether it fits the person sitting in the room.
Psychodynamic Psychotherapy: Working in Depth
Psychodynamic psychotherapy is the approach I offer. It has its roots in the earliest forms of talking therapy and has evolved considerably, shaped significantly by female clinicians and researchers who brought relational, embodied, and social dimensions of trauma into focus. Judith Herman’s model of trauma recovery, Valerie Sinason’s work on dissociation and split-off parts of the self, and the Tavistock approach developed by Jo Stubley and colleagues have all contributed to a contemporary psychodynamic practice that looks quite different from its origins.
In psychodynamic work, the aim is not symptom reduction alone but a deeper understanding of how trauma has shaped your inner world, your relationships, and your sense of self. Some of what that involves:
- Working with all parts of the self. Trauma often causes aspects of experience to become fragmented or cut off. These might appear as strong feelings, numbness, bodily reactions, or distinct internal states. Rather than pushing these aside, psychodynamic therapy brings them into the work, with the aim of greater integration over time.
- Making the unbearable thinkable. Trauma can leave experiences that feel impossible to put into words. The therapeutic space is designed to make it possible to approach what has felt overwhelming, not by forcing a narrative, but by creating enough safety for meaning to develop gradually.
- Using what happens between us. The patterns and feelings that developed in early or traumatic relationships tend to show up in the therapeutic relationship itself. Rather than treating this as a complication, psychodynamic therapy uses it as live material, noticing what emerges between us and opening up new possibilities for relating.
- Attending to the body and the unconscious. Dreams, physical states, sudden reactions, and what goes unsaid all carry information about experience that hasn’t yet found language. Psychodynamic work pays attention to these signals rather than filtering them out.
- Supporting durable change. By working through the layered and often hidden effects of trauma, people frequently find that change extends beyond symptom relief into how they experience relationships, themselves, and their capacity to be present in their own lives.
- This approach is particularly well-suited to complex, relational, or longstanding trauma, where what’s needed is depth and integration rather than a time-limited protocol.
This approach is especially valuable when trauma has been repeated, relational, or longstanding.
Stages of Trauma Therapy
Judith Herman’s influential model of trauma recovery, first set out in Trauma and Recovery (1992), describes three broad stages of therapeutic work. These aren’t a rigid protocol or a ladder to climb in sequence. They’re a framework for understanding what the work involves and why it tends to unfold the way it does.
Stage One: Safety and Stabilisation. Before anything else, the work focuses on establishing enough internal and external safety to make deeper exploration possible. This might involve building capacity to manage overwhelming emotions, developing grounding skills, establishing a stable therapeutic relationship, and addressing any immediate risks or practical circumstances that are making life unmanageable. For some people this stage takes months. For others it takes considerably longer, and that’s appropriate rather than slow. Trying to process traumatic material before sufficient stability is in place tends to be counterproductive and can increase distress rather than reduce it.
Stage Two: Remembrance and Mourning. Once there is enough stability, the work can move toward the traumatic experience itself. It’s important to be clear about what this does and doesn’t mean. Stage two is not about excavating every detail of what happened, constructing a complete narrative, or systematically revisiting the past. Research suggests that detailed recall of traumatic events is not necessary for meaningful therapeutic progress, and pushing for it can be actively unhelpful. The work is more accurately described as attending to what is coming up now, the feelings, physical responses, relational patterns, and fragments of experience that are present in the room, and working with those as they arise. What needs to surface tends to surface when the conditions are safe enough. The therapist’s role is to work with what appears rather than to go looking for what doesn’t.
Stage Three: Reconnection and Integration. As the weight of the past begins to shift, the focus moves toward rebuilding a life that isn’t organised around the trauma. This might involve re-engaging with relationships, revisiting identity, developing a sense of future, and consolidating the changes that therapy has made possible. It’s less about processing and more about living.
A Few Things Worth Knowing
These stages don’t move in a straight line. It’s entirely normal to return to stabilisation work during stage two when something particularly difficult surfaces, or to find that reconnection brings up material that needs further processing. Progress in trauma therapy is rarely linear, and moving back through an earlier stage isn’t failure. It’s the work responding to what’s actually needed.
It’s also normal to take breaks between stages, sometimes extended ones. Life intervenes. Capacity fluctuates. The therapeutic relationship may naturally reach a resting point at the end of one stage, and returning for the next stage later, whether with the same therapist or a different one, is a legitimate and well-recognised pattern. Different therapists bring different strengths, and the person best suited to stabilisation work isn’t always the same person best suited to deeper processing or integration. Changing therapist between stages, or returning to a previous therapist for a later stage, doesn’t mean the earlier work failed. It means you’re making an informed choice about what you need now.
.
Other Ways of Working With Trauma
Psychodynamic therapy isn’t the only effective approach to trauma, and it isn’t the right fit for everyone. The following are established approaches with their own evidence bases, each working somewhat differently.
Trauma-Focused Cognitive Behavioural Therapy (TF-CBT) works primarily from the top down, helping to identify and modify distorted beliefs and avoidance patterns connected to traumatic experience. It has a strong evidence base for single-incident trauma and PTSD, and tends to be more structured and time-limited than psychodynamic work.
EMDR (Eye Movement Desensitisation and Reprocessing) uses bilateral stimulation alongside focused attention on traumatic memories to reduce their distressing charge. It has good evidence for single-incident PTSD and some evidence for more complex presentations, particularly when combined with stabilisation work.
Internal Family Systems (IFS) works with a model of internal parts, each understood as having its own perspective and protective function. It’s worth knowing that parts language isn’t new to psychotherapy. Psychodynamic and object relations traditions have worked with fragmented and dissociated aspects of the self since the mid-twentieth century, through the work of Fairbairn, Winnicott, Sinason, and others. IFS offers a structured framework for similar territory, though its research base is currently limited compared to longer-established approaches. It is also practised by therapists and coaches across a wide range of orientations and training backgrounds, so it’s worth checking credentials carefully if you’re considering it. The IFS Institute directory (ifs-institute.com) lists trained practitioners.
Sensorimotor Psychotherapy and Somatic Experiencing work directly with the body, tracking physical sensation and movement as primary routes into traumatic experience. These are clinically distinct from general physical practices and require specialist training. They can be particularly useful where trauma is held predominantly in the body or where verbal processing alone hasn’t been sufficient.
Art therapy uses image-making, drawing, painting, and other visual processes as the primary medium of therapeutic work rather than talk. It is particularly useful where verbal expression feels limited or where trauma has been stored in ways that don’t readily translate into language. Art therapists in the UK are regulated by the Health and Care Professions Council (HCPC) and hold postgraduate-level training.
Sandtray therapy invites clients to create scenes using miniature figures and objects in a tray of sand, allowing unconscious material to surface in symbolic form without requiring verbal articulation. It has roots in Jungian analytic practice and is used with both adults and children. It can be particularly valuable for early or pre-verbal trauma where language-based approaches have limited reach.
Music therapy uses structured musical experience, including improvisation, listening, and songwriting, as a therapeutic medium. Like art therapy, it is HCPC-regulated in the UK and requires postgraduate training. It is less commonly encountered in private practice than in clinical and educational settings, but can be a powerful route into emotional experience for people who find music a more accessible medium than words.
Therapeutic writing and creative therapies more broadly offer routes into experience that bypass the verbal and cognitive channels where trauma can be most defended. I integrate therapeutic writing into my trauma work when appropriate and requested.
Group therapy provides something that individual therapy cannot: the experience of being witnessed and accepted by peers, of discovering that your experience is not as singular as it may have felt, and of healing within a relational context that mirrors ordinary life more closely than a one-to-one setting.
Complementary and body-based practices including yoga, tai chi, mindfulness, drama therapy, and ecotherapy or nature-based approaches such as gardening, are sometimes used alongside formal therapy rather than as standalone treatments. They are not clinical modalities in the same sense as the approaches above, but they can support nervous system regulation, grounding, and a sense of connection to self and environment. Drama therapy, like art and music therapy, is HCPC-regulated in the UK and sits closer to clinical practice than the others in this group. If any of these appeal to you, they work best as a complement to rather than a replacement for trauma-focused therapeutic work, particularly where trauma is complex or longstanding.
Many people find it helpful to combine approaches, for example, body practices alongside
psychodynamic talking therapy.
Choosing What’s Right for You
There is no single therapy that works for everyone, and finding the right approach may involve some exploration. The questions worth asking any prospective therapist include: what training do you have specifically in trauma? How do you approach the body in your work? What happens if I dissociate in a session? How do you think about the therapeutic relationship itself?
My way of working isn’t the only way, and it may not be what you need right now. If another approach feels more relevant to your situation, that’s worth following. My hope is that this guide helps you understand what’s available and gives you better questions to ask as you look.
If you’d like to explore whether psychodynamic therapy might be a good fit, I’d be glad to have an initial conversation. Get in touch at samanthamerry.co.uk/contacts.
References
Herman, J. L. (1992/2015). Trauma and Recovery: The Aftermath of Violence, From Domestic Abuse to Political Terror.Basic Books.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the Body: A Sensorimotor Approach to Psychotherapy. W. W. Norton.
Paintain, E., & Cassidy, S. (2018). First-line therapy for post-traumatic stress disorder: A systematic review of cognitive behavioural therapy and psychodynamic approaches. Counselling and Psychotherapy Research, 18(3), 237–250.
Sinason, V. (1994). Mental Handicap and the Human Condition: New Approaches from the Tavistock. Free Association Books.
Spermon, D., Darlington, Y., & Gibney, P. (2010). Psychodynamic psychotherapy for complex trauma: Targets, focus, applications, and outcomes. Psychology Research and Behavior Management, 3, 119–127.
Stubley, J. (2010). Attachment and trauma: Working relationally with survivors of extreme experiences. In Relational Trauma: A Contemporary Introduction (Eds. P. Hughes & J. Baylin). Routledge.
Van Nieuwenhove, K., & Meganck, R. (2020). Core interpersonal patterns in complex trauma and the process of change in psychodynamic therapy: A case comparison study. Frontiers in Psychology, 11, 122.
Samantha Merry is a BACP Senior Accredited Psychotherapist in private practice in Bromley, South East London, and a doctoral researcher at the University of Chester.
Footnote: Historical and Contemporary Context
Psychodynamic psychotherapy is not a fixed tradition but an evolving set of ideas and practices. While its roots lie in early psychoanalysis, the field has moved far beyond Freud’s time.
Much of this development has been led by women clinicians and researchers, who have emphasised the relational, embodied, and social dimensions of trauma. Judith Herman’s influential model of recovery, and the Tavistock approach shaped by Jo Stubley and colleagues, highlight the importance of safety, relationship, and the capacity to think about overwhelming experiences. Valerie Sinason draws attention to dissociation and the presence of split-off parts of the self, an area where psychodynamic therapy has long worked, welcoming all aspects of the self whether they appear as distinct “parts,” bodily states, or unconscious processes.
These perspectives align with newer insights from body-oriented approaches such as sensorimotor psychotherapy, which recognise how trauma is held in somatic states as well as in mind. Contemporary research supports the ongoing value of psychodynamic psychotherapy in working with complex trauma, and services such as the specialist Trauma Service at the Tavistock and Portman NHS Foundation Trust continue to draw on
psychoanalytic and psychodynamic practice as part of evidence-based care.